
ACTS THAT KILL AND ACTS THAT DO NOT — A PHILOSOPHICAL ANALYSIS OF THE DEAD DONOR RULE Download PDF
Cheng-Chih Tsai (Center for Holistic Education, MacKay Medical College)
© 2021 Cheng-Chih Tsai
DOI: https://doi.org/10.31820/ejap.17.1.4
Original scientific article – Received: 12/10/2020 Accepted: 15/05/2021
ABSTRACT
In response to recent debates on the need to abandon the Dead Donor Rule (DDR) to facilitate vital-organ transplantation, I claim that, through a detailed philosophical analysis of the Uniform Determination of Death Act (UDDA) and the DDR, some acts that seem to violate DDR in fact do not, thus DDR can be upheld. The paper consists of two parts. First, standard apparatuses of the philosophy of language, such as sense, referent, truth condition, and definite description are employed to show that there exists an internally consistent and coherent interpretation of UDDA which resolves the Reduction Problem and the Ambiguity Problem that allegedly threaten the UDDA framework, and as a corollary, the practice of Donation after the Circulatory Determination of Death (DCDD) does not violate DDR. Second, an interpretation of the DDR, termed ‘No Hastening Death Rule’ (NHDR), is formulated so that, given that autonomy and non-maleficence principles are observed, the waiting time for organ procurement can be further shortened without DDR being violated.
Keywords: DDR; UDDA; DCDD; NHDR; vital organ; causation
Introduction
In the practices of vital-organ transplantation, while doctors typically want to procure a vital-organ as early as possible, the Dead Donor Rule (DDR) requires them to wait till the donor is dead, for otherwise the procurement would constitute, presumably, an act of killing. For some authors (cf. Veatch 2008), this amounts to the impossibility of a lawful vital-organ transplantation. Commenting on this situation, Robert Truog maintains that current practices in organ procurement do cause the death of the person if death is understood in the ‘scientific way’,[1] and claims that while the long-term solution to this problem should be to reframe the ethics of vital-organ donation in terms of the principle of respect for autonomy and the principle of non-maleficence rather than the DDR, the short term solution is to “conceptualize current approaches to defining death as socially acceptable ‘legal fictions’”[2] (Truog 2015, 1885). Walter Sinnott-Armstrong and Franklin Miller (2013), on the other hand, offer a more radical solution by showing that there is nothing wrong with killing per se, hence DDR can be safely dropped.
The present paper proposes an alternative way out. By resorting to standard apparatuses in the philosophy of language and putting DDR and other relevant regulations or practices, such as UDDA and DCDD, under scrutiny,[3] I show that there is an interpretation of UDDA that captures a certain aspect of our intuition about the death of a person,[4] and, with respect to which, current practices of DCDD do not violate DDR. Hence there is neither a short-term need to regard UDDA as merely creating legal fictions nor a long-term need to abandon DDR. More specifically, I discuss two conceptual problems which, with DDR upheld, seem to threaten the present definition of UDDA and current practices of organ transplantation,[5] and resolve them in philosophical terms. Then I go one step further to formulate NHDR (No Hastening Death Rule), a version of DDR, which I claim to capture the spirit of donor protection better than the DDR taken at face value, and with NHDR, the waiting time for an organ procurement can be further shortened.
1. Upholding DDR in the Face of UDDA
By the Dead Donor Rule (DDR), I mean the following:
DDR A vital organ H of a person A can be procured for donation at time t only if A is already dead at t.
Here, I should clarify what I mean by a ‘vital organ’ first. A ‘vital organ’ can mean a type of organs the removal of which would generally lead to the death of the owner. Heart, for example, is a vital organ in this sense, while appendix is not. However, a ‘vital organ’ can also denote a specific organ of a person the removal of which would lead to the person’s death. Although heart is a vital organ in the first sense, a specific heart might not be vital in the second sense if its owner will be blown to pieces by a bomb a split second later or if its owner is currently receiving a new heart through a heart transplantation—after all, the removal of the (old) heart would not in any way hasten his death. To avoid further confusion, I shall refer to a vital organ in the first sense by a ‘vital-organ’, and reserve the term ‘vital organ’ for a vital organ in the second sense, and throughout Section 1, we shall only understand the ‘vital organ’ in DDR in the first sense, namely, as “vital-organ”. In other words, in Section 1, we are concerned with
[DDR1] A vital-organ H of a person A can be procured for donation at time t only if A is already dead at t.
In general, interpreting DDR in the first sense would yield us a rule which is more strict, because, according to it, insofar as an organ is a vital-organ, it can only be procured after the owner is dead, even if the organ is actually not vital for that person.[6] In this section, issues about the UDDA-DDR framework and the practices of vital-organ procurement in the US will be formulated as two conceptual problems, which will then be settled by linguistic and philosophical means.
1.1 The Reduction Problem—How can Death Amount to Brain Death?
In Truog (2007), it says that in 2005, Dr. Sanjay Gupta, a neurosurgeon and Senior Medical Correspondence for CNN, told Larry King, “Well, you know, a dead person really means that the heart is no longer beating […] people do draw a distinction between brain dead and dead” (Truog 2007, 274), which amounts to publicly disagreeing with current medical and legal criteria of death. Indeed, some authors, such as D. Alan Shewmon and Robert D. Truog, have tried and succeeded in convincing key figures in medical ethics, including some members of the President’s Council on Bioethics,[7] to the extent that the Council admits that “[…] it would be difficult to deny that the body of a patient with total brain failure can still be alive, at least in some cases” (Miller and Truog 2011, 72).
In this subsection, we discuss whether it is justifiable to define the death of a person in terms of the ‘death’ of one of his or her organs. Now, the death statement ‘John is dead’ clearly cannot be defined by ‘The brain of John is dead’. The subject of the former sentence, namely ‘John’, is a proper name referring to a person, while that of the latter, namely ‘the brain of John’, is a definite description denoting an organ, yet they share the common predicate ‘dead’. Apparently, we cannot define the death of something in terms of the death of some other thing if we do not know the extension of ‘death’ in the first place.
A natural solution to the above problem is to stress that the phrase ‘brain-death’ itself by no means suggests that the death of a person is characterized by the ‘death’ of his brain; it only suggests that the death of a person is to be determined by some condition of his brain. For example, using ‘b-death’ instead of ‘death’ for the brain condition in question is a way out. To avoid future confusion, let me introduce new symbols to stand for some predicates that concern us in this paper.
- ‘John is D’ stands for ‘John is dead’.
- ‘John is Db’ stands for ‘John is brain-dead’.
- ‘The brain is bD’ stands for ‘the brain is b-dead’.
The brain-dead definition of death can then be summarized as follow:
John is D if John is Db, and John is Db if the brain of John is bD. (*)
While the subject of a sentence of the form ‘John is D’ is still a proper name that refers to a person, and the criterion for the person’s death is still expressed in terms of a sentence whose subject is a definite description, namely ‘the brain of John’, which denotes the brain of the person, the latter sentence is no longer a statement about the death of a “person”, and the predicate is bD instead of D or Db.
Note that regardless of what the content of bD truly is, the presence of a definite description in (*) alone generates a semantic issue concerning personal death. As ‘John is D’ is about John, while ‘the brain of John is bD’ is about John’s brain, it is unlikely that the two sentences can be synonymous.[8] Intuitively, if John loses his entire brain, then we would say that John is dead. Nevertheless, the bD statement about John’s brain now becomes either truth-valueless (analogous to the claim that ‘the King of France is bald’ makes no statement when there is simply no King of France at present) or false (if Russell’s theory of definite description is to be adopted).[9] So, the practice of defining the death of a person in terms of certain property of some part of the person’s body seems problematic. Following the spirit of a Strawson/Wolfram framework,[10] which regards ‘the King of France is bald’ as making no statement, one can claim that if John has lost his brain then a sentence token ‘John is D’ is truth-valueless. On the other hand, according to the Russellian framework, if John has no brain then he cannot be D, which is even more absurd. Imagine trying to complete a sentence that begins with “Pew is blind if and only if the eyes of Pew are …”, while soon reckoning that it is possible that Blind Pew simply has no eyes.
Elbourne claims that for certain sentences in which definite descriptions are embedded under propositional attitude verbs and conditionals, the Fregean analysis of definite descriptions is superior to the Russellian analysis. For example, “Hans wants the ghost in his attic to be quiet tonight” (Elbourne 2010, 8) does not entail that Hans wants that there exists exactly one ghost in his attic[11] (the Russellian way). Rather, it presupposes the existence of exactly one ghost in his attic (the Fregean way). Similarly, “If the ghost in his attic is quiet tonight, Hans will hold a party” is not to be rephrased as “If there is exactly one ghost in his attic and it is quiet tonight, Hans will hold a party” (Elbourne 2010, 2). Again, it presupposes the existence of exactly one ghost in his attic.
This framework helps us to better analyze the problem that I raised two paragraphs back. Analogous to Elbourne’s analysis,[12] the sentence ‘John is D if and only if the brain of John is bD’ is not to be translated as ‘John is D if and only if there is exactly one brain of John and it is bD’. John’s having a brain is no longer a necessary condition for his death. Rather, (*) only presupposes the existence of a brain of John and when John has lost his brain, (*) is no longer applicable. What can we say about John’s death if at the instance of his death he does not have a brain?[13]
Recall that the Fregean account of sense and reference tells us that the sense of ‘John’ in ‘John walks’ determines the referent [John]w of ‘John’ when the sentence is tokened in world w, and the token is true provided that [John]w lies in [walks]w, the set of all things that walk. Would such a mechanism work for a death statement of the form ‘John is dead’ as well? At the most abstract level, it would still work, but in practice it does not. If John is blown into pieces by a bomb, then there simply is no entity left in the world that can be said to be the ‘referent’ of ‘John’, but we can still claim that he is dead. Presumably, outlining the truth condition of a death statement without assuming that ‘John’ refers is a better approach. According to this approach, we only need to resort to something denoted by the definite description ‘the brain of John’ and see if it lies in the extension of the predicate bD. More specifically, the no-brain (or no-body) problem mentioned earlier can be resolved by 1) taking the definite description ‘the brain of John’ as presupposing the existence of a unique referent rather than asserting its existence, and 2) in case John has lost his brain (or his entire body), we simply stipulate that he is dead because his brain no longer exists—in other words, ‘the brain of John is bD’ vacuously holds. So, in contrast to the Russellian account, the brain of John is bD if and only if John has exactly one brain and the brain meets the criteria associated with bD or John no longer has a brain. Specifically, when John has lost his brain, the sentence ‘John is D’ is false, truth-valueless, and true according to the Russellian account, the Fregean account, and the present account, respectively.
In sum, despite that the subject of ‘John is dead’ is a proper name for a person, the truth condition of the statement can be described by another sentence whose subject is a definite description denoting one specific organ of John. Here the definite description itself is to be interpreted more in the Fregean than in the Russellian way. However, when the definite description fails to denote, the death statement will still have a definite truth value, rather than remains undecided.
1.2 The Ambiguity Problem—Do We Have Two Distinct Notions of Death?
In 1981, The Uniform Determination of Death Act (UDDA) was approved as a model state law for the United States. It states that an individual who has sustained either (1) irreversible cessation of circulatory and respiratory functions, or (2) irreversible cessation of all functions of the entire brain, including the brain stem, is dead. Furthermore, a determination of death must be made in accordance with accepted medical standards.
A general concern now arises.
(i) The death + death = life Problem
If UDDA is understood as a definition, which defines D as the disjunction of Dh and Db, where Dh is a short-hand for the state of a person who meets (1), while Db is a short-hand for the state of a person who meets (2), then we immediately encounter the alleged death + death = life problem. To be more precise. Let A be one that is Dh already but not yet Db, and B be one that is Db already but not yet Dh. According to UDDA, they are both dead, but given that the transplantation option is available, can we not make use of A’s brain and B’s heart-lung system and build a living being from two dead persons?
This is not as problematic as it sounds. Imagine that a certain creature, Two-Eye say, is composed of a left eye and a right eye. A Two-Eye is impaired if at least one of its eyes is broken. Then if recombination is possible, we can surely expect to get a non-impaired Two-Eye from a pair of impaired Two-Eyes. After all, the problem is with personal identity rather than with life-and-death.
If neither the brain nor the heart-lung system is essential[14]—that is, they are replaceable—then the resulting living individual should neither be A nor be B, as they are both dead already, and dead people are not expected to come back to life. But as the Two-Eye case demonstrates, there is nothing odd here at all.
If the brain is the essential part of a person, however, then the resulting living individual should of course be A. But, isn’t A already dead by UDDA? How come he/she comes back to life after the transplantations? Shouldn’t this prove that UDDA is problematic? Not really! The point is that if clause (1) is to be considered as a sufficient condition for death, and it involves irreversibility in its terms, then to announce the death of A before the transplantation, we should have thought of the possibility of transplantation. Given that after the transplantation, A is apparently alive, we should realize that the prior announcement of the death had been premature—A’s circulatory and respiratory functions were not yet “irreversibly-ceased” in the first place. So, there is no death + death = life problem for us to worry about here.
Alternatively, we can regard UDDA as merely listing two criteria of death, which together characterize death, rather than regarding each of clause (1) and clause (2) as semantically capturing the essence of death. For example, if we follow the idea that what is essential for a person is his/her brain, and what is essential for a person’s life is his/her brain function, then UDDA amounts to characterizing the brain condition of a person through two criteria which are pragmatically, rather than semantically, related to the underlying condition of the brain.
For brevity and clarity, I will introduce the following abbreviations. If clause (1) of UDDA is met, I shall say that the person’s brain is bD1, and if clause (2) of UDDA is met, I shall say that the person’s brain is bD2. UDDA recognizes the irreversible cessation of all functions of the entire brain, i.e. bD2, as a criterion for death, which allows doctors to procure vital-organs from Db (brain-dead) victims without violating the Dead Donor Rule. However, with the acceptance of UDDA, Donation after the Circulatory Determination of Death (DCDD) can be a protocol for vital-organ donation as well: the life support equipment for severely brain damaged patients are removed until the patients meet the traditional circulatory and respiratory criteria for death and then the organs are removed.
Now, the listing of these two distinct criteria for death in UDDA makes the concept of death sound ambiguous and compromising. In particular, on the face of it, one can be dead without her brain being bD2—meeting the criterion of bD1 suffices —which seemingly contradicts the guiding principle that D (death) is characterized by Db (brain-death), which in turn is the main driving force of UDDA’s coming to being.
More specifically, we can imagine that[15] (a) while John’s brain is still functioning, some foreign creature rips his heart and lung out from his chest in an instant, and, Dr. Who, who is obsessed with brain research, happily takes this chance and pronounces John dead based on the fact that John’s circulatory and respiratory functions have irreversibly ceased, and immediately procures John’s brain for research. Intuitively we would expect that as John’s brain can still work for a split second after his heart and lung are ripped away, he is not dead yet and Dr. Who is doing harm to a living person rather than merely manipulating the corpus of a dead man.
Analogously, we can imagine that (b) John’s brain has met the bD2 dead criterion but his heart is still beating strongly for unknown reasons. Some people may find it difficult, as Dr. Gupta did, to suppress the intuition that John is not dead yet,[16] despite that John has met the criteria of death prescribed by UDDA.
A natural reaction to the above objections would be to reformulate UDDA. However, UDDA is the outcome of the collective wisdom of many individuals, and has been in use for several decades. So, despite that there are issues that need to be dealt with more carefully—especially the conceptual ones like the ambiguity problem I have just mentioned—insofar as these issues can be adequately explained in linguistic/philosophical terms, our priority should be in keeping it rather than altering it. Now, as we have seen in the previous subsection, while a death statement concerns a person, its truth condition only resorts to some particular organ of the person. So, there can be no ambiguity problem in UDDA at all. Clause (1) and clause (2) collectively characterize the condition of death for an individual—in our terms, John is D iff John’s brain is bD, and John’s brain is bD iff John’s brain is either bD1 or bD2—and so long as one of the clauses holds, the person is dead. In other words, ‘John is still alive’ amounts to the conjunction of two clauses.
With the help of these two notions of bD1 and bD2, we can observe that, our daily uses of the term ‘brain-death’ can actually mean two different things. It can mean either that John’s brain is bD or that John’s brain is bD2. However, please bear in mind that in this paper the term ‘brain-death’ is reserved for the first reading only.
Now, recall that scenario (a) seems more disturbing than scenario (b). So far as scenario (b) is concerned, nowadays many surgeons have been practicing the procurement of a beating heart from a person whose brain meets the bD2 criterion, without feeling that the donor is still alive. It appears that the concept of the death of a person can be a constructed idea that we can gradually adapt to. Can one’s uneasiness towards scenario (a) be similarly resolved in the future? The answer is probably ‘no’.
In defining death, many authors have attempted to resort to higher brain death,[17] or the so called ‘cerebral death’, instead of the whole brain death. It reflects the fact that John Locke’s psychological continuity account of personal identity is not something that easily fades. On the one hand, higher brain death proponents maintain that the whole brain death, or the bD2 criterion, is not necessary for the death of a person. On the other hand, they may suspect that the irreversible cessation of circulatory and respiratory functions, or the bD1 criterion, is not sufficient for the death of a person, as the higher brain may still be functional. The latter is precisely the concern that my scenario (a) tries to raise: is it possible that a person who is still conscious, hence alive, be mistakenly pronounced dead according to clause (1) of UDDA?
A brain’s being bD is the disjunction of its being bD1 and its being bD2, thus the application condition of bD2 is, in practice, more strict than that for bD—otherwise we would not need the other criterion, namely, bD1, in the first place. So, a brain can indeed be bD without being bD2, as the higher brain death proponents would have maintained. However, given that we only have two criteria of death, can the other criterion, namely bD1, truly capture the higher brain death so that the person in scenario (a) would not be mistakenly pronounced dead?
Note that the bD1 criterion, like the bD2 criterion, serves as an indication that the brain of the person is bD.[18] However, the bD2 criterion normally takes longer to meet than the criterion for the bD1 criterion. In practice, the bD2 test is usually done when the heart-lung system is still working (with the help of an artificial life support system, if needed) so it involves a long period of waiting time before checking for brain activities for a second time, while the bD1 test is usually done when the heart-lung failure is imminent and it involves a waiting time of only several minutes. The hidden consensus here is that if the circulatory and respiratory functions have ceased for that amount of time, the brain would have been in the state of bD even though we have not gone through the usual bD2 test procedure for it.[19]
In sum, the cessation of circulatory-respiratory functions can indeed be seen as a sign that indicates that the brain of the individual in question is bD already. While we may not have the means to directly assess the condition of the brain, we may still pronounce the patient dead according to the bD1 criterion, because without the help of an artificial life support, the cessation of the circulatory-respiratory function is a sure sign that the ‘key’ brain functions would cease in several minutes if nothing is to be done about it. So, the list of two criteria of death in UDDA itself does not make the notion of death ambiguous. A truth condition may come with two criteria, and insofar as the criteria collectively shape the right concept, the listing of two criteria causes no harm.
Now, back to scenario (a). Taking the above into account, what can we say about it? In (a), the heart and lung of John are ripped away in an instant, so, on the face of it, his circulatory and respiratory functions have irreversibly ceased, thus he has met the first clause of UDDA and can be pronounced dead, which seems to contradict our intuition that he is not dead yet. However, remember that in this particular scenario, we have not gone through the waiting time of several minutes as required by accepted medical standards. So, we cannot say that the bD1 has been met or that the brain is already bD. As the story has already suggested, John might still have a split second of consciousness left after his heart and lung were ripped away, thus the instant ripping away of John’s heart/lung does not entail his death right away—the usual several minutes of waiting is still needed for us to pronounce that the brain of John is bD1.
This indeed safeguards human life. Recall that all the issues concerning DDR, UDDA and DCDD etc. arise because of the possibility of vital-organ transplantation. Now, even though John’s original heart-lung system has been ripped away, there is still the possibility that, with the most advanced medical technology, a new heart-lung system can be transplanted into John’s chest and begin to function in less than a minute’s time, just before John’s brain is forever damaged. In other words, ‘the circulatory and respiratory functions of the heart-lung system of John’ cannot be said to be irreversibly lost at the time of ripping, because that definite description ‘the heart-lung system’ denotes a system of John that is in his chest (or somewhere nearby), regardless of whether it is the original one or a replacement. When we say that the president of America has always been male, we by no means mean that Joe Biden has always been a male. Rather, we mean that each president of America has been male to date. Analogously, to say that the heart-lung system of John has irreversibly ceased functioning, we should ensure that no possible replacement heart-lung system, such as an artificial heart-lung system, or a new heart-lung system with a transplanted heart, can succeed as ‘the heart-lung system of John’[20] and function properly, and this necessitates the waiting of several minutes before the pronouncement of death. So scenario (a) amounts to a premature judgement of death. John was not dead yet immediately after the ripping away of his heart-lung system—his brain was neither bD2 nor bD1 yet, even though his original biological heart-lung system had indeed irreversibly ceased to function.
Another alleged problem related to the ambiguity problem is the following.
(ii) The Reversing the Irreversible Problem
While the Denver case of successful heart transplantation was hailed as a great medical achievement, Veatch draws our attention to the fact that the procurement of hearts from DCDD patients for organ donation seems to involve reversing the irreversible (Veatch 2008). Imagine that a critically ill patient John has chosen to forgo life-sustaining treatment and donate his heart. After the withdrawal of life-sustaining equipment, his heart stops and after several minutes of waiting, he is pronounced dead because his circulatory and respiratory functions are regarded as irreversibly lost, and his heart is procured and transplanted into the chest of another patient, Smith say, who was on ECMO and has been waiting for a new heart for some time. Smith lives well after the transplant, which implies that the new heart is beating well in his body. Now, according to Veatch’s insight, a moment ago it was declared that the circulatory and respiratory functions of John’s heart-lung system were irreversibly lost, and now the heart is beating again in another person’s body, does this act of transplantation not amount to reversing the irreversible?
Veatch’s point sounds convincing, and according to this view, the Denver doctors were guilty of procuring vital organs before the donor was dead, thus had violated the homicide law by killing the donor for his or her heart. But, as this act saved the lives of the organ recipients, we may choose to just muddle through. Or, alternatively, we can see the death of the donor as just a legal fiction: the donor is not really dead yet, but based on UDDA and current medical criteria for bD1, the donor is ‘dead’ already, even if the donor’s heart actually beats nicely in another person’s chest later. Possible solutions to Veatch’s challenge, other than muddling through or regarding UDDA as creating legal fictions, include 1) deleting the first criterion of UDDA or disallowing the procurement of hearts from patients who seemingly have (but in fact have not) met the DCDD criterion hereafter, because these patients are not dead yet, and procuring their vital-organs violates the DDR; 2) not altering UDDA but simply dropping the DDR, thus allowing the procurement of vital-organs from patients who seemingly have (but in fact have not) met the DCDD criterion; 3) replacing the ‘irreversibility’ requirement of UDDA by ‘permanence’ so that, insofar as the procurement is performed, the person’s circulatory and respiratory functions have ceased permanently, hence he is dead regardless of whether the organ is reversible.
We will not consider options 1) and 2) as they involve either dropping UDDA or abandoning DDR, and the goal of the paper is to show that they can be held without inconsistency. We will not accept 3) either, because it literally alters UDDA—namely, by replacing ‘irreversible’ by ‘permanent’. Nevertheless, in Section 2, I will return to 3) and see it as a failed attempt to shortening the waiting time for a death pronouncement. In the meantime, I would only stress that with the help of a careful linguistic analysis of the predication of ‘irreversible’, we can show that there is no ‘reversing the irreversible’ involved in DCDD donation in the first place.
The following example prepares us for this point. Imagine that an alien creature needs two functional hearts, an L-heart and an R-heart, for it to be alive. So both hearts are vital for such creatures. Now, the function of an L-heart will be irreversibly lost after it stops beating for 4 minutes and the function of an R-heart will be irreversibly lost after it stops beating for 2 minutes. Furthermore, an R-heart will stop beating after its corresponding L-heart has stopped beating for 2 minutes, and similarly, an L-heart will stop beating after its corresponding R-heart has stopped beating for 2 minutes. So a creature can be pronounced dead after its L-heart has stopped beating for 4 minutes or after its R-heart has stopped beating for 2 minutes. Moreover, while an L-heart is transplantable, an R-heart is not. Now, suppose Alice is such a creature, and the function of her L-heart has stopped beating for 4 minutes. Can we transplant Alice’s L-heart into Betty’s body without violating the DDR? Yes, because Alice is already dead by the criteria set for these creatures, yet the transplanted L-heart still has a chance of beating again inside Betty’s body. If the transplantation is successful, and Alice’s original L-heart is now beating again in Betty’s body, are we not reversing the irreversible? Surely not. What is irreversibly lost is the function of the L-heart in Alice’s body—the stopping of the L-heart for 4 minutes has implied that the corresponding R-heart has stopped for 2 minutes, which in turn implies that its corresponding L-heart, in Alice’s body, will not be functioning again. It says nothing about the function of the L-heart in Betty’s body.
The fact that the L-heart of Alice is irreversible at the time of procurement and the fact that the L-heart of Betty is beating afterward[21] do not contradict each other, even though the former is spatial-temporally continuous with the latter (they are virtually the same heart). In conclusion, there is no ‘reversing the irreversible’ problem at all.
Now, back to our case concerning DCDD. The irreversibility of John’s circulatory and respiratory functions is, after all, a property of John rather than of a particular heart/lung system, while the beating again of the donated heart is merely a property of the heart, and these facts do not contradict each other. John’s failing to have his circulatory-respiratory functions re-established on site reveals the fact that he is brain-dead in the sense that his brain is b-dead, but that does not imply that his former heart-lung system cannot be functional in another person’s body.
To sum up this section, the criteria of death listed in UDDA help materialize the truth condition of a death statement, by drawing our attention to the conditions of some suitable organ of an individual. When it comes to the pinning down of the semantics of a death statement, all we need is a way of finding out whether some portion of a body can be considered as the brain of the individual, and whether the circulatory and respiratory functions of a heart-lung system or all functions of the entire brain are irreversibly lost. Finally, brain-death says more about the non-existence of a functioning brain than about the existence of a non-functioning brain.
2. Reinterpreting the Dead Donor Rule—The No Hastening Death Rule
In this section, we explore the possibility of understanding the ‘vital organ’ in DDR in the second sense, and show that with this interpretation, the waiting time for procurement can be further shortened without the rule being violated. In particular, we shall adopt Shewmon’s insight concerning the interpretation of DDR, develop it into a more workable version, and show that certain seemingly hasty procurements of vital-organs are not killing acts at all.
2.1 Causing Death as Hastening Death
In the Conclusion section of Shewmon (2004), we find:
“Regarding organ transplantation, the important and truly meaningful question is not ‘When is the patient dead?’ but rather ‘When can organs X, Y, Z … be removed without causing or hastening death or harming the patient in anyway?’” (Shewmon 2004, 297, Emphasis added)
More explicitly, in Shewmon, and Shewmon (2004, 110), we see:
“[…] This approach to heart/lung retrieval does not cause or hasten death, because once circulation has effectively ceased due to the effect of progressive hypoxia on the heart, the dying or decaying process continues just the same regardless whether the nonbeating heart and nonfunctioning lungs remain physically in the circulationless body or not.” (Shewmon, and Shewmon 2004, 110, emphasis added)
Note that in these passages, Shewmon wrote as if ‘causing death’ and ‘hastening death’ amount to roughly the same thing. However, we will see that, depending on how we conceive of causation, while the two notions can indeed be interchangeable if a specific but-for styled account of causation restricted to the causation of death is adopted, they can also mean radically different things according to other accounts, such as according to a version of NESS[22] which regards the death of A as some event incorporating all details of the way the death comes about.
For simplicity of treatment, I shall define the vitality of an organ in terms of ‘causing death’ first, and then identify ‘causing death’ with ‘hastening death’ as Shewmon seems to have suggested, only after a particular notion of death causing is subscribed later.
Recall that in this section we shall understand the ‘vital organ’ in DDR in the second sense. As a consequence, by Contraposition and some other elementary logical rules, DDR can be rephrased as
[DDR2] If A is not already dead at t, then an organ H of a person A can be procured for donation at time t only when H is not vital then.
Now, defining vitality of an organ in terms of ‘causing death’, we have
[Vitality] An organ H of A is vital at t if the procurement of H from A at t would cause A’s death,
As the DDR is clearly a rule concerning the living rather than the dead, and for a dead person no organ is vital, the antecedent of [DDR2] can be dropped, and then [DDR2] and [Vitality] can be combined into a single rule.
[*] An organ H of a person A can be procured for donation at time t only if the procurement of H would not cause A’s death.
This is a decent rule. However, what exactly do we mean by ‘causing of a death’ here and what are the causal relata in question?[23] While this paper is no place for us to review a full range of accounts of causation and give the causation in question a particular theory-laden interpretation, we can at least consider two standard accounts of causation, namely the counterfactual account of David Lewis and the NESS account of Richard W. Wright, and see whether they are up to the job of characterizing the causation in [*].
Recall that the counterfactual account of causation faces the challenge of pre-emption. Take the famous Suzy and Billy throwing rock scenario for example. Suzy and Billy both threw a rock at a bottle, Suzy’s rock hit the bottle first and broke it. Intuition seems to suggest that Suzy’s throwing the rock is the cause of the breakage of the bottle. Nonetheless, according to the counterfactual theory of causation, had Suzy not thrown the rock, the bottle would have been broken by Billy’s rock, so Suzy’s throwing of the rock is not the cause. This is counter-intuitive.
The NESS account solves the problem by reckoning that while Suzy’ throwing a rock is not a but-for cause, it is indeed a necessary element of a set of conditions sufficient for the breakage of the bottle. So Suzy’s throwing is a NESS cause of the breakage. Nevertheless, according to this account Billy’s throwing a rock is a NESS cause as well. This is counter-intuitive too.
To solve the counter-intuitive conclusions mentioned above, the counterfactual theorist and NESS theorist often resort to the fact that by examining the way the bottle was broken to pieces one can establish that the underlying causation at work is Suzy’s rock breaking the bottle rather than Billy’s rock breaking the bottle. In other words, by fine-graining the effect, so that ‘the breakage of the bottle’ contains more details about how it is broken, both the but-for test and NESS test remain plausible accounts of causation.
Hereafter, I will apply a time-frame analysis to (1) the rock-throwing case, (2) a famous hypothetical of McLaughlin and (3) the organ procurement case, which is the primary concern of this paper, and show that there is a better strategy dealing with the causation of death than indefinitely fine-graining the effect.
We start with an analysis of a but-for statement. In saying that but for the procurement of H, A would not have died, we surely do not mean that but for the procurement of H, A would live forever. Rather, we seem to have a time frame such that at some time t~>t, both the procurement of H and the death of A has happened, at t and t respectively, with t>t, and had the procurement of H not occurred, the death of A would occur at some other time t> t~. The problem here is that this reference time t~ seems arbitrary—being the time the discourse takes place.
Applied to the rock-throwing case, the time frame can be illustrated as in Figure 1.
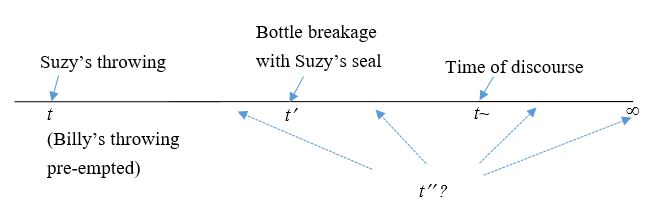
Figure 1. The Rock-Throwing Case
We have the following candidates for a but-for account based on the location of t—the time of the breakage of the bottle had Suzy not thrown the rock.
- [But-for 1] t = But for Suzy’s throw, the bottle would never be broken
- [But-for 2] t > t~ But for Suzy’s throw, the bottle would still be unbroken at the time of discourse.
- [But-for 3] t > t But for Suzy’s throw, the bottle would still be unbroken at t.
- [Fine-grained] The location of t is irrelevant, even t < t is acceptable. What matters is Suzy’s signature/seal in the breakage.
Now, as the primary concern of this paper is not a general account of causation, we will be content with applying the above framework only to the causation of death. In that case, option 1) and 2) are to be ruled out right away as, first, even if the procurement had not been carried out, the death of patient would have been bound to happen at some later time, and, second, an organ donation case can be reviewed at any time and there is no apparent reason why the discourse time should play a role, despite that a but-for statement usually, on the face of it, takes the form of “… would not have happened”.
Option 4) is more subtle and it seems to capture many, if not most, people’s intuition. As long as a high-speed camera captures the detail of the breakage of the bottle and reveals that it’s Suzy’s rock that is involved in the physical process of the breakage of the bottle, then some would think it’s Suzy’s rock throwing that caused the breakage, even if had Billy’s throwing not been pre-empted by Suzy’s throwing, Billy’s rock would have broken the bottle at a time t earlier than t.
I would not try to challenge this intuition here, but would rather draw the reader’s attention to the following scenario adopted from a famous hypothetical of McLaughlin, which is discussed in McLaughlin (1925) and Moore (2009). A man, Dan say, was to travel to the desert with a bottle of water. Before he set off, one rival of his, Bob say, added poison to the water, intending to kill him, while an hour later, another rival of his, Sue say, without knowing what Bob had done, emptied the bottle, also intending to kill Dan. Dan died of thirst in the desert in the end. Now, what was the cause of his death?
According to a coarse-grained but-for test, both rivals’ acts aren’t but-for causes for Dan’s death, while according to a coarse-grained NESS test, both rivals’ acts are NESS causes. Yet, according to a finer-grained but-for test, Sue’s act is the cause of Dan’s death by thirst, because but for Sue’s act, Dan would not have died of thirst. On the other hand, according a finer-grained NESS test, Bob’s act isn’t the NESS cause of the death of Dan, because adding poison cannot be said to be a necessary element of a set of conditions sufficient for Dan’s death by thirst. The scenario can be summed up in the following way (see Figure 2).
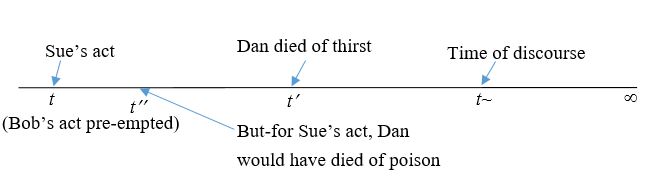
Figure 2. The Water Keg Case
Note that while, indeed, but for Sue’s act, Dan would not have died of thirst, and Sue’s act alone is a necessary element of a set of conditions sufficient for Dan’s dying of thirst, we can consider the following twist of the story before asserting that Sue’s act is the cause of Dan’s death. Suppose, that Sue was not a rival of Dan, and she knowingly emptied the bottle to avoid Dan’s being poisoned by Bob. Having no clean water to refill the bottle, Sue had done her best to save/prolong the life of Dan. It is simply ridiculous to say that her act is the cause of Dan’s death.
Now, many theorists assume that actual causation is a factual causation[24], but, if that is true, then the fact that we are reluctant to deem Sue’s act a cause of Dan’s death after learning the mindset of Sue together with the fact that the twist of the story does not affect the underlying physical facts represented in the picture should prompt us to have a second thought about embracing 4).
Finally, back to our original context, I propose that, instead of embracing 4), we adopt 3), and the procurement of H causes, or more straightforwardly hastens, the death of A only when t > t, as shown in Figure 3.
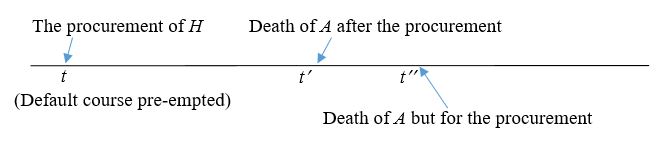
Figure 3. A Death-Hastening Procurement
As a consequence of this account, if t < t, then even if the death of A does bear the signature of procurement, we cannot say that the procurement of H causes the death of A, after all, it prolongs life rather than hastens death. We then arrive at a new version of DDR, which can be term NHDR (No Hastening Death Rule)
NHDR If a person A is to donate his/her organ H then the procurement of H should not hasten A’s death.
Note that as vitality is understood as hastening death through procurement, NHDR amounts to the slogan: ‘No Vital Organ Procurement!’. This partly explains why people, such as Veatch, are tempted to suspect that DDR cannot be consistently held in the practices of vital-organ transplantation. However, as we have repeatedly stressed, vital-organs are not necessarily vital organs, and a vital-organ H can by all means be non-vital for A yet becomes a vital organ for B after the transplantation. There is no problem with the slogan.
Before we look more closely at how the NHDR scheme works in the practice of organ procurements, we need to digress for a while to discuss an issue relevant to the re-formulation of DDR, so as to be better prepared for the analysis. Recall that we mentioned earlier that replacing ‘irreversibility’ by ’permanence’ in the definition of death can shorten the waiting time for vital-organ procurements so that an organ can be procured well before it is damaged (Bernat 2013). However, this amounts to either changing UDDA or violating the DDR, because permanence does not imply irreversibility. After all, irreversibility is a modal property, which involves a set of possible worlds, but permanence only concerns the actual world. Irreversibility is a state of an entity which is characterized by its possible behaviors at various possible worlds, but permanence is not. To say that something has irreversibly lost some feature that it once exhibited, we need only to look at its current state and then, by consulting past statistics and predictions by experts, assert the irreversibility. But to say that the lost is permanent, we are talking about a four-dimensional continuum which constitutes the world line of the individual, therefore we can pass judgement without resorting to past statistics or future predictions about people in similar conditions. We simply need to check the whole continuum of an individual and find out whether the feature indeed never reappears. A patient whose heart has stopped but has not yet met the irreversibility criteria of UDDA—for example, the required several minutes’ waiting time has not yet elapsed—may actually be ‘permanently-dead’ because no one attempted to resuscitate him. Therefore, permanence does not entail irreversibility.
On the other hand, it is imaginable that a patient who has been pronounced dead based on the irreversibility requirement of UDDA can be brought back to life by a miraculous divine action. Thus irreversibility[25] does not entail permanence either.
The advantage of the move to replace ‘irreversibility’ by ‘permanence’ in UDDA is of course that no doctor would be accused of procuring the heart from a heart stopping donor whose heart has not met the permanence requirement of death, because the doctor’s act of procurement itself would guarantee that no heart would ever be beating again in the chest of the donor. But this move is in practice unacceptable, because it will allow an ER staff who is reluctant to perform CPR to a heart stopping patient to defend himself/herself by saying that “the heart-beat monitor be my witness, at the time of the patient’s arrival, his heart has stopped permanently”.
However, sticking to the irreversibility requirement of UDDA would, as Bernat (2013) stresses, allegedly increase the waiting time before procurement, because biological irreversibility generally comes much later than the irreversibility judged by current medical technology. Furthermore, modern medicine has made ECMO a standard equipment in major hospitals, thus theoretically a heart stopping patient cannot be declared dead before ECMO has been tried. But such waiting is in most cases unnecessary, a waste of resource, and even harmful to the patient and her family. What can we say about this? I think, as John Lizza has elaborated in Lizza (2005), irreversibility needs qualification. We have, to name just a few, logical irreversibility, metaphysical irreversibility, physical irreversibility, biological irreversibility, technological irreversibility, situational irreversibility (imagine you have a heart attack in the middle of the Sahara desert), and societal irreversibility (imagine you have signed a DNR[26]) etc. How is the irreversibility in UDDA to be understood?
Biological irreversibility seems to be a nice candidate. However, taking into account the conjecture that life on earth starts as a result of a coincidental lightning strike to a suitable earth environment,[27] there is always a chance that a dramatic event would bring a heart stopping patient back to life. Therefore, biological irreversibility is an unrealistic, even vacuous, notion to be considered as the underlying interpretation for irreversibility involved in the UDDA. In contrast, a notion of irreversibility based on a social-norm which takes biological, technological, situational, and legal considerations all into account can turn out to be more realistic. For a general account about how social norms can play a significant role in the ethics of killing, see Tsai (2017).
Now, back to the main concern of this section. I claim that without taking the move to replace irreversibility by permanence, NHDR itself allows us to shorten the waiting time for the procurement of a heart that has stopped beating—especially when we have had the consent from a donor who very much liked to donate his or her heart, and we can make sure that the anesthesia will be properly administrated during the operation (so that autonomy and non-maleficence that Troug (2015), cares about will be safeguarded) without violating DDR. The details are as follows.
2.2 Alternative Ways of Dying
Recall that in contrast to hasty DCDD (the procurement of a stopping heart without waiting long enough to ensure irreversibility), treatment-withdrawal with DNR has become an acceptable practice in many societies today. In other words, a dying patient can ask for the withdrawal of the life sustaining equipment and dying as a consequence, and no member of the medical staff would be accused of killing the patient by shutting down the life-sustaining system. On the other hand, the procurement of a heart that has stopped beating without waiting for several minutes to make sure that the heart of the donor has met the irreversibility criterion is disallowed as it violates [DDR1].
However, if NHDR is adopted instead, then a hasty DCDD does not always violate DDR. To decide whether such an act of procurement violates DDR, we are to see whether the act hastens death, by comparing the times of death associated with the procurement and the non-procurement (the default) respectively. In Figure 4, compare the following value-time diagrams of a case of treatment-withdraw with DNR and a case of hasty DCDD.
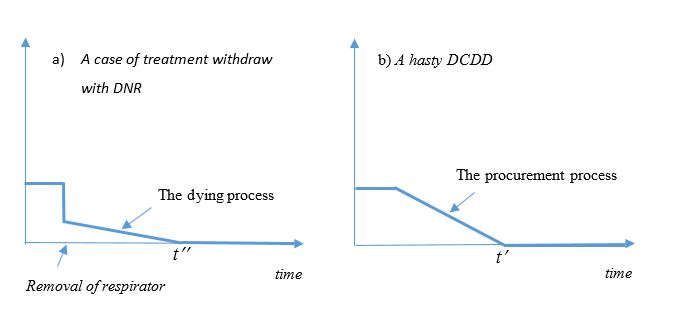
Figure 4. Two Ways of Dying
In case that autonomy and non-maleficence are both guaranteed, there is no reason why a) is allowed while b) is disallowed. Judged from the graphs, a) and b) are both processes from life to death. They are simply two ways of dying. And so far as death time is concerned, the procurement does not hasten death insofar as t t, so it does not violate NHDR. After all, in the case of a hasty DCDD for a patient with DNR, while it is hasty in the sense that the donor is not dead yet, so long as t t, it does not hasten death, and thus what has been procured is not a vital organ and NHDR has not been violated.
If nowadays we can accept, unlike some decades ago, that removing a life support device does not always constitute an act of killing, we should accept that a hasty DCDD does not necessarily constitute an act of killing as well. When one has decided to be let die and does not mind which course her dying process will take, death by treatment-withdrawal with DNR and death by DCDD really make little difference.
The analysis scheme above is new but its conclusion—namely, hasty DCDD is not always wrong—is by no means new, as it has long been observed in Shewmon (2004) and Shewmon and Shewmon (2004). Nevertheless, the analytic scheme of this paper indeed grants us an easy and a principle-based way to explain why certain seemingly unacceptable acts are actually acceptable, as the following imaginary scenario demonstrates.
A criminal has jumped from the top of a 101-story building to seek death. He will be dead in a few seconds. Before he hits the ground, he is offered a final chance to payback to society. With his consent, a cushion will be provided to delay the death, and a hi-tech ultra-fast snatcher can procure his heart from his chest a split second before he eventually hits the ground, and the heart can then be used to save someone’s life soon after. If he agrees to the proposal, do we commit homicide by procuring his heart right before he crashes? Is his heart really a vital organ then? Will DDR be violated?
The answers to the last three questions are clearly, I suppose, all ‘no’ as suggested by Figure 5.
Figure 5. A Non-Killing Procurement
3. Conclusion
Let me sum up what we have achieved in this paper, by reviewing some of the claims in Marquis (2010) which maintains that DCDD donors are not dead. There Marquis claims that DCDD proponents often ‘appeal to permanence’ or ‘appeal to a norm’ to show that DCDD donors are dead, but the two appeals both fail. In Section 1, I have stressed that irreversibility and permanence are different things, so we should not substitute permanence for irreversibility and appeal to permanence. Similarly, substituting norm for irreversibility and then appealing to norm won’t work either, as criteria in UDDA are clearly biological in nature. Therefore, we agree with Marquis that the two appeals he addresses in his paper indeed fail. However, that does not imply that DCDD donors are not dead. It only shows that proponents of DCDD often appeal to wrong items. In Section 1, I have, without appealing to either permanence or norm, shown that so long as UDDA are properly understood and obeyed, DCDD donors are dead already within the scheme. Furthermore, in Section 2, I have shown that so long as autonomy and non-maleficence principles are observed, some hasty DCDDs — i.e. procurements done before DCDD donors are dead — can be compatible with a newly interpreted DDR too.[28]
Acknowledgments
I would like to thank three anonymous reviewers of this journal for insightful criticisms and constructive suggestions that helped me turn this paper into a solid and consistent piece of work. Thanks are also due to other reviewers that have previously commented on earlier versions of this paper. A special thank is due to Yi, Fu-Yun, for being the sole audience of a draft presentation upon which the current paper was developed, and her comments were very much appreciated.
The work was supported in part by the Ministry of Science and Technology, Taiwan [grant numbers MOST 102-2410-H-715-001-MY3 and MOST 107-2410-H-715 -004 -MY3]. The author is obliged.
REFERENCES
Bernat, James. L. 2013. ‘On Noncongruence between the Concept and Determination of Death’. Hastings Center Report 43 (6): 25-33.
Brugger, E. Christian. 2013. ‘D. Alan Shewmon and the PCBE’s White Paper on Brain Death: Are Brain-Dead Patients Dead?’ Journal of Medicine and Philosophy 38 (2): 205–218.
DeGrazia, David. 2005. Human Identity and Bioethics. Cambridge: Cambridge University Press.
Elbourne, Paul. 2010. ‘The Existence Entailments of Definite Descriptions’. Linguistics and Philosophy 33 (1): 1-10.
Hess, Benjamin L., Sandra Piazolo, and Jason Harvey. 2021. ‘Lightning Strikes as a Major Facilitator of Prebiotic Phosphorus Reduction on Early Earth’. Nature Communications 12 (1): 1535. https://doi.org/10.1038/s41467-021-21849-2
Joffe, Ari. 2018. ‘DCDD Donors Are Not Dead’. Hastings Center Report 48 (6): S29-S36.
Lizza, John P. 2005. ‘Potentiality, Irreversibility, and Death’. Journal of Medicine and Philosophy 30 (1): 45-64.
Lizza, John P. 2011. ‘Where’s Waldo? The “Decapitation Gambit” and the Definition of Death’. Journal of Medical Ethics 37 (12): 743-746
Marquis, Don. 2010. ‘Are DCD Donors Dead?’ Hastings Center Report 40 (3): 24-31.
McLaughlin, James Angell. 1925. ‘Proximate Cause’. Harvard Law Review 39 (2): 149-199.
McMahan, Jeff. 2002. The Ethics of Killings: Problems at the Margins of Life. Oxford: Oxford University Press.
Miller, Franklin G., Robert D. Truog, and Dan W Brock. 2010. ‘The Dead Donor Rule: Can it Withstand Critical Scrutiny?’ Journal of Medicine and Philosophy 35 (3): 299-312.
Miller, Franklin G., and Robert D. Truog. 2011. Death, Dying, and Organ Transplantation: Reconstructing Medical Ethics at the End of Life. New York: Oxford University Press.
Moore, Michael S. 2009. Causation and Responsibility: An Essay in Law, Morals, and Metaphysics. New York: Oxford University Press.
Paul, Laurie Ann, and Edward J. Hall. 2013. Causation: A User’s Guide. Oxford: Oxford University Press.
Shewmon, D. Alan. 2004. ‘The Dead Donor Rule: Lessons from Linguistics’. Kennedy Institute of Ethics Journal 14 (3): 277-300.
Shewmon, D. Alan. 2010. ‘Constructing the Death Elephant: A Synthetic Paradigm Shift for the Definition, Criteria, and Tests for Death’. Journal of Medicine and Philosophy 35 (3): 256-98.
Shewmon, D. Alan, and Elisabeth Seitz Shewmon. 2004. ‘The Semiotics of Death and its Medical Implications’. In, Brain Death and Disorders of Consciousness. Advances in Experimental Medicine and Biology, Vol. 550, edited by Calixto Machado and D. Alan Shewmon, 89-114. New York: Kluwer Academic/Plenum Publishers.
Sinnott-Armstrong, Walter, and Franklin G. Miller. 2013. ‘What Makes Killing Wrong?’ Journal of Medical Ethics 39 (1): 3-7.
Truog, Robert D. 2007. ‘Brain Death – Too Flawed to Endure, Too Ingrained to Abandon’. Journal of Law, Medicine and Ethics 35 (2): 273-281.
Truog, Robert D. 2015. ‘Defining Death: Getting It Wrong for All the Right Reasons’. Texas Law Review 93 (7): 1885-1914.
Tsai, Cheng-Chih. 2017. ‘Killing, a Conceptual Analysis’. Ethical Perspectives 24 (3): 467-499.
Veatch, Robert M. 2008. ‘Donating Hearts after Cardiac Death—Reversing the Irreversible’. New England Journal of Medicine 369: 672-673.
Veatch, Robert M. 2010. ‘Transplanting Hearts after Death Measured by Cardiac Criteria: the Challenge to the Dead Donor Rule’. Journal of Medicine and Philosophy 35 (6): 313-329.
Wolfram, Sybil. 1989. Philosophical Logic, An Introduction. London and New York: Routledge.
Endnotes
- The scientific standard mentioned in Truog (2015), attributed to Bernat, defines death as “the permanent cessation of functioning of the organism as a whole” (Truog 2015, 1892). ↑
- By regarding a current definition of death as merely a ‘legal fiction’, one is reluctant to accept that the definition has captured the true notion of death. ↑
- These are the abbreviations for the ‘Uniform Determination of Death Act’, and ‘Donation after the Circulatory Determination of Death’ respectively. ↑
- Shewmon (2004; 2010) nicely demonstrates the intrinsic difficulties in obtaining a uniform definition of death. ↑
- See Veatch (2008; 2010) for example. Note that many authors have proposed that DDR should be revised or dropped, see, for instance, Miller, Truog, and Brock (2010) and Sinnott-Armstrong and Miller (2013). ↑
- Certainly, in rare cases, a non-vital-organ can happen to be vital for a particular person as well, whose procurement will be blocked by the DDR in the second sense but allowed by the DDR in the first sense. But, for simplicity, we shall ignore such cases in this paper. ↑
- See President’s Council on Bioethics: Controversies in the Determination of Death 2008. ↑
- In the sense that the truth condition of one is governed by the other. ↑
- According to Russell’s theory, for the b-death statement to be true, John has to have a brain to start with. More specifically, the F is Q if and only if (i) there is an x such that Fx, (ii) for all y, if Fy then x=y, and (iii) Qx. ↑
- See Wolfram (1989). ↑
- For simplicity, here I assume that ‘Hans wants A and B’ implies ‘Hans wants A’. ↑
- Note that Elbourne’s analysis is primarily for embedded statements, but we find an analogous phenomenon here. ↑
- Strictly speaking, when John has gotten two brains, (*) is inapplicable also. ↑
- Here by ‘essential’, I mean essential of for personal identity, not essential for life. ↑
- See Lizza (2011) for a treatment of this problem through the example of decapitation. ↑
- Shewmon, Truog, and a minority of the President’s Council would be reluctant to accept that John is already dead as well. See for example, Brugger (2013). ↑
- See DeGrazia (2005) and McMahan (2002). ↑
- In Bernat’s words, “the circulatory criterion is valid only because it leads to the brain criterion” (Bernat 2013, 28). ↑
- I do not claim that this notion of brain-death and the ‘higher-brain-death’ amount to the same thing. But it is certainly plausible. ↑
- Note that here the de dicto, or small scope, reading of the definite description is the intended interpretation, otherwise vital organ transplantation would not be possible in the first place. ↑
- Note that (the function of) Betty’s L-heart cannot be said to be irreversible before the transplantation. The L-heart may be not functioning before the transplantation, but with the transplantation option, it is not irreversible yet. ↑
- NESS is a short for Necessary Element in a Set of conditions Sufficient for the effect. See, for instance, Moore (2009) and references therein for how it works. ↑
- See Hall and Paul (2004) and the references therein. ↑
- See Moore (2009) for the repeated emphasis on this. ↑
- People usually presuppose some practical constraints on reversibility. For example, if the story of Jesus’ raising Lazarus is true, we would still regard Lazarus’ state as dead before the raising, because under “normal” conditions a person in that state has no chance to be brought back to life. ↑
- A shorthand for ‘Do Not Resuscitate’. ↑
- For instance, see Hess, Piazolo, and Harvey (2021). ↑
- Ari Joffe also claims that DCDD donors are not dead in Joffe (2018), in which four reasons that death is not merely permanent are given and three common objections to this idea are refuted. Again, I agree with him that substituting permanence for irreversibility is a bad idea. However, DCDD donors can be dead on the irreversibility criteria alone (Section 1), and my new interpretation of DDR can even allow some hasty DCDDs (Section 2). ↑